
Myofascial Trigger Points - Helping to Unravel the mystery of pain
There are many ways to place your body under stress. This can occur as a macrotrauma (e.g. whiplash, road traffic accident, sports injury, surgery) or microtrauma (e.g. prolonged poor posture) which itself can be contributed to by emotional stress and tension.
The myofascial system is your connective tissue network of fascia and muscle that forms an interconnecting web supporting the human body. It also provides a conduit (or pathway) for movement, transport of lymph and nutrients.
Restriction with formation of trigger points will lead to pain, restricted range of movement and potentially an array of other symptoms as diverse as headaches, seizures, numbness, autonomic dysfunction, genital pain, and dizziness. It has been reported that up to 85% of pain in a general practice setting is caused by trigger points (Cummings and White, 2001).
What is a Trigger Point?
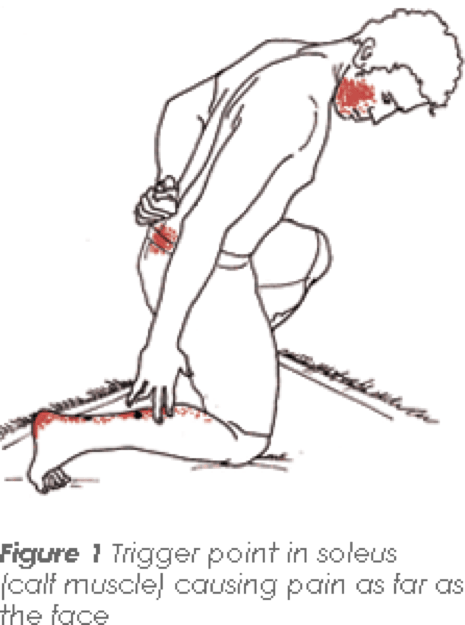
A trigger point is an area of hyperirritable muscle that when pushed creates a regional aching pain. It can be palpated (or felt) as a taut band. The pain does not follow a neural, dermatomal pattern created by aggravation of a nerve root and often the pain will be distant from the source of the trigger point. Six hundred and twenty Trigger Points have been identified and documented with specific referral patterns. The early work was conducted over many years by two Drs: Dr Janet Travell (Physician to John F Kennedy) and Dr David Simons.
Are We Able To Visualise Trigger Points?
Mainstream x-ray/MRI will not show trigger points but other types of advanced imaging have:
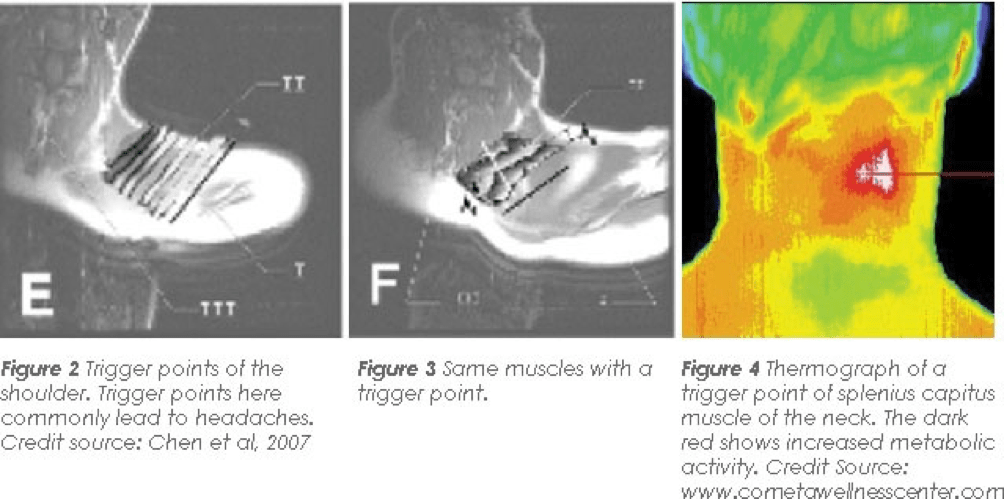
Figure 2 shows a normal alignment of muscular fibres in the trapezius muscle. Figure 3 shows the same muscle with a trigger point.
How Are These Treated?
Conventional stretching is not advised for treatment of these trigger points as you are likely to stress a muscle already under stress and compound the problem. The first step is a complete evaluation by a healthcare practitioner such as a Physiotherapist or Osteopath who will identify the problem. From this point forwards techniques vary. The most common is direct pressure followed by a gentle stretch to recover normal muscle length. Other methods include laser therapy, dry needling and PNF/muscle energy techniques.
Treating The Underlying Cause
The immediate relief from a release can be short lived if the underlying cause is not treated. Sometimes this is a joint dysfunction, which can be eased with mobilisation and often it will be an ergonomics issue that your therapist can advise you on and provide exercises to help correct.
Following traumatic injuries such as whiplash, before a trigger point is treated, joints that need to be stabilised will be stabilised through strengthening, otherwise treatment would be unsuccessful and possibly detrimental (Thompson, 2001).
Nutrition
As integrative practitioners we realise that there is often a nutritional component to pain.
Dr Travell and Simons also noted that almost half of their patients required treatment for vitamin inadequacies to obtain lasting relief from the pain and dysfunction of trigger points, and thought it was one of the most important perpetuating factors to address. They prioritised B-1, B-6, B-12, folic acid, vitamin C, and the minerals calcium, magnesium, iron and potassium. The deficiencies in these vitamins cause hyper irritability of the nervous system and may also contribute to neuropathic (nerve) pain. In early Carpel Tunnell syndrome for example there is some evidence that a B6 deficiency can significantly contribute to pain.
Patients presenting with a low-normal blood test should still be wary. To maintain adequate blood levels of a nutrient, your body will pull nutrients from the tissues leaving you with hidden deficiency. Furthermore blood tests conducted are not always reflective of the true situation. Common (serum testing) of Magnesium for example only reflects about 0.3% of the bodies total magnesium and patients have been found to be deficient in the red blood cell despite normal serum levels.
Summary
Pain is complex, the remarkable distribution of trigger point type pain only complicates that picture. A skilled practitioner however is able to discern a potential myofascial pain syndrome and seek the origins of the discomfort thorough a knowledge of referral patterns and careful evaluation and palpation.
Whilst some patients may only require a couple of symptomatic treatments, for many a thorough examination of causative factors are required for long lasting relief.
References:
Alvarez, D.J., Rockwell P.G. (2002) Trigger Points: Diagnosis and Management. Fam Physician. Feb 15;65(4):653-661
Chen. Q et al (2007) Identification and quantification of myofascial taut bands with magnetic resonance elastography. Ach Phys Med Rehabil 88:1658-1661
Thompson B 2001 Neuromuscular massage therapy perspective. Journal of Bodywork and Movement Therapy 5(4): 229-23